
We put out a call on facebook in mid-July for questions from locals about the coronavirus pandemic. Here is first the post, which accompanied an image of our "We Are All In This Together -- Whether We Admit It Or Not" article, and then a compilation of what people asked and our responses:
OP: This column goes over in more detail why there is so much urgency over masks. Just saying that you have a right to do what you please without wearing a mask impacts the entire community or takes a chance that it could, even if you haven't had a problem yet. Yes, if we had more widespread testing to monitor transmission, we might be able to declare a given area to be less susceptible and people could be more relaxed, but we don't know what our current status is, really. We only know how people in our area were faring as of a couple weeks ago. It's a constant gamble.
(To be clear, no one knows this information; it's not that it is some kind of secret knowledge. There's just a lag in the time it takes for the disease to be transmitted, run its course, and possibly be transmitted again before it surfaces in the numbers. That's why extensive testing or even sentinel testing of wastewater could help, allowing for identification of community spread without waiting for symptoms to show.)
So, in the absence of up-to-the-minute information and given a deep-seated desire to be able to support local businesses and go about as much of our lives as we possibly can, we need everyone to get on board with mitigation. As President Trump and the US Surgeon General said earlier this week: "We're asking everybody that when you are not able to socially distance, wear a mask."
There is still so much anger and confusion about this. If people have specific questions about COVID-19, masks, other mitigation measures, reading the statistics, testing, rumors, or other related topics, we would be glad to help you find answers.
More on the president's call for universal masking.
QUESTION 1: Meme posted saying, we have to stay inside forever so no one ever dies.
ANSWER 1: It is true that locking down is one way of reducing transmission. It’s also clear that that is not indefinitely viable. Or desirable. That said, the last time we locked down, it was by no means comprehensive and arguably, we squandered the time we bought in the process, which could have been used to ramp up production of materiel like PPE and ventilators, build out our testing and tracing capacity, and develop protocols for regional and national logistical response. We did not do these things. At this point, we are trying to reduce the R value by other means, including a combination of masking, distancing, and hygiene on the part of individuals and businesses and organizations and a combination of testing, tracing and treatment at a broader level. If we cannot keep disease spread under control, however, shutting down again may become necessary. Long term, we are hoping to get a ringer in the R value game, by developing a vaccine. The point is: in order to be able to open and stay open, we need to do things like wearing masks, practice distancing, and upping hygiene. Can we get on board to do that or must we stay stuck in a counterproductively defiant mode, posting hostile memes?
QUESTION 2 (comments from three different people): I guess I would ask how we measure things. If the goal is to get to 80%, what percentage are we at now, and how do we know? How do we measure the spread here locally as attributed from non-mask wearing? Spain and Italy have many more deaths per million than the US, for example, and they have over 80% of people say they wear a mask whenever they leave their home, so there must be other factors at play besides just the masks, and i'm sure those factors contribute here as well. I'm also not sure of the facts on the local increase she references. According to the NYT, both Union and Northumberland counties are pretty stable with their new case counts over the past two weeks. Yes, there are new cases. But its also a time when people are traveling. If masks were the end all, I believe we would have much greater spread by now.
I guess you could start by looking around when you go to businesses. Is everyone properly masking? Is everyone unmasked? Does it seem like an even mix? If everyone who can wears their mask, we all benefit. And regarding Italy and Spain, seems like they’ve made tremendous progress since their first “peaks” in the spring, truly flattening their curves. I take that as evidence that this whole masking thing really does work...or they would be looking like us. Seems like the people who take huge issue with it, globally, are Americans. And our curve is sure reflecting that!
so is the 80% based on looks? I'm just asking how we get to our goal. It seems like most people mask when working or going in businesses, but then don't when they are in social situations (based on my observations around town). Spain's new case chart looks exactly like Pennsylvania's as far as the curve goes, and both Spain and Italy's death charts are similar to ours, so I'm not sure what you mean by "looking like us." I'm fine with wearing a mask inside and if I was in a crowded place outside, I just think there are other factors to be considered as well. I don't believe we will ever get to a point where everyone locally will wear one when they leave their house unless it becomes a punishable offense because a. people are skeptical of information that has changed so drastically, and b. people aren't afraid due to the low case/death numbers. Again, I'm just speaking of the general public around here, not myself.
Oh I’m talking about the US in general. Thankful for some of the early measures our governor took here to mitigate its spread. And this is the kind of thing I’m looking at re: cases and how terribly we’re doing as a nation rn:
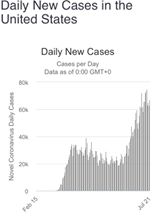
Vs Spain 🇪🇸 https://www.worldometers.info/coronavirus/#countries

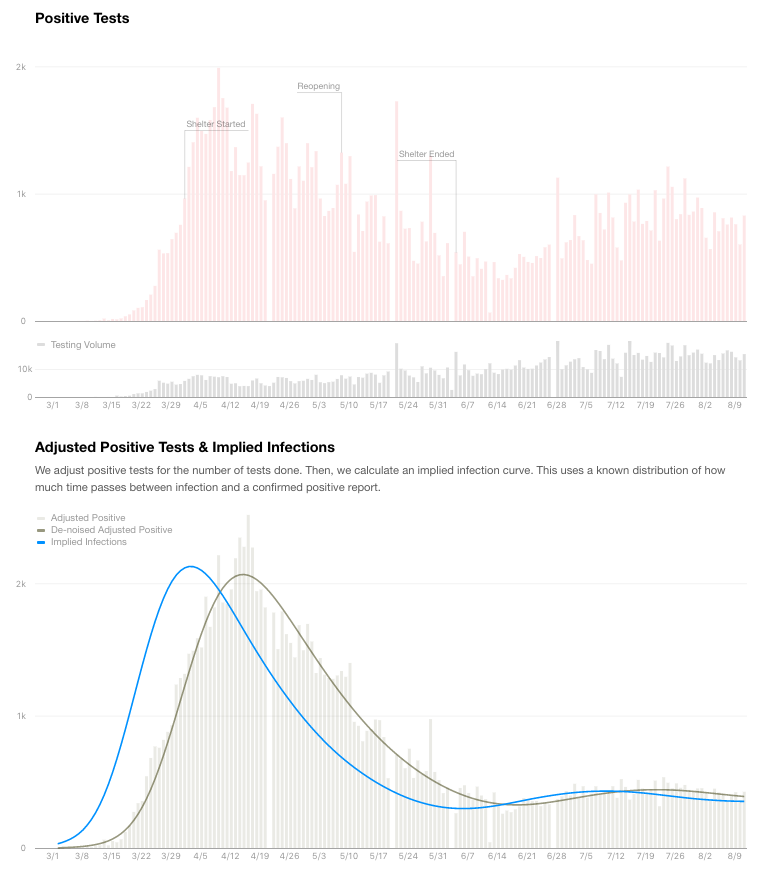
Our death rate is not rising, according to the pa department of health and the NYT. Our seven day average for daily deaths has been between 17 and 28 from June 21 to July 21st, with the 17 being July 20 and 21st. I agree PA is comparable to Spain and Italy, thats why I brought them up, because they are reporting around 85% of people saying they wear a mask every time they leave their house. Again I don't think that kind of measurement has been done here. If it had, and we were also at 85%, then we could say masks are working in both places. But, I believe the implication of the article is that we are below the 80% needed to be effective against community spread. So why are we similar to a place that has above that? There may be more to it than masks. I totally hear you about school, its so frustrating! My son is definitely suffering from the lack of being able to see friends and family.
here’s the chart to illustrate your point about PA death rates.

ANSWER 2: There are a whole lot of separate questions here. About how we count things, how we know things, and how we compare to other places. In terms of assessing the number of people actually masking and how many are needed, this article offers some insights in lay terms and this is the specific scientific article that came to the 80% adoption of 60% effective masks: https://www.theatlantic.com/health/archive/2020/04/dont-wear-mask-yourself/610336/ and https://arxiv.org/pdf/2003.07353.pdf respectively. You will note that they come up with this as a range and conclude that if the masks were 100% effective, you would only need about 40% of the population wearing them and vice versa, if 100% of people were wearing them, they would only need to be 40% effective. It's not like it's 80% and no more, we need at least 80%. If there are more people, that just means we are reducing the R value faster/further.
As to how you assess how many people are wearing them, is the question how to count this? Having traveled to Massachusetts in mid-July, it was patently obvious that more people are wearing them there. It's still not full compliance and people are not wearing them when distanced, for example on the beach… It would not be that difficult to conceive of a system of assessing compliance. Hong Kong is estimated to have 98% mask wearing.
There has also been some published polling about how many people are wearing masks in different countries, but that leaves things open to the wide variation in different parts of the country (not to mention how the questions are phrased). We are clearly in a pocket where fewer people wear masks than could and where as of yet we have not had much disease transmission. At the same time, it's not as if our infection rate has been zero; until the end of July it had been a remarkably steady rate of about 5 cases/day in the four county area (Snyder, Union, Northumberland and Montour) for the past 3 months. Apparently the mitigation measures that have been in place including the shut down and people just voluntarily being more distanced has kept us to that steady trajectory. We are now faced with the challenge of a significant increase in connection and potential exposure in the form of school reopenings, both public schools and universities, and are trying to implement a mitigation measure that will allow for the increased exposure without also resulting in an increasing rate of case growth.
Looking at how our numbers compare to Spain, in fact, it is true that our per capita cases and deaths as a state are quite close to their numbers, but you will also see that they had a more extreme rise to start and a more effective reduction, going down to what would have been proportionally a third of the level our new cases per day dropped to. You will also see that Spain's case numbers are starting to rise again, though not yet to the per capita rate we have returned to. It's also critical to note that as a result the country is now cutting back on nightlife, restaurants, and bars, and even locking some regions back down. In other words, Spain's curve, while similar in overall shape to ours, shows that they had done a more effective job than we have with disease suppression and, though their numbers had not rebounded proportionally as much as ours, they have taken action to further reduce spread.
As to why we look to have similarly reduced our cases here in PA, masks are not being proposed as the "be all" by any stretch of the imagination. They are one tool in the toolbox available to us for use in our efforts to reduce transmission. Other tools included the shut down, but at least in theory if we can implement masking more extensively, we would be able to reopen without having the numbers starting to tick back up. So, why did PA's curve drop like Italy's and Spain's even without us masking? At least initially, we were largely shut down. We had also closed our schools, which create fairly dense networks of interconnection within the community and, through the universities, bridge our small town isolation and connect us more to the rest of the country. So, with the school closures, we had significantly reduced exposure and therefore transmission. Now we want to increase connections but still keep the transmission low, so we need to use multiple other tools, chief among them masks, distancing, and hygiene. We can also use policies that have to do with whether we can visit other states with more spread and, if we choose to do so, make sure that people self-isolate upon return. The long term goal for the reduction of the R value is a vaccine. That is another piece of the puzzle, but one we are still waiting for. In the meantime, we use the tools we do have, including masks.
As to the PA death rate remaining low right now even though confirmed cases are rising. There are several factors here. Probably the most significant is the concept that we probably undercounted cases by so much back in April that the current rise is not as great in comparison to the first peak as it might seem. By using the test positivity rates it is possible to reconstruct what the actual case count probably was previously. Seen in that context our rising count right now is actually more a question of catching more of the cases, but the death rate seems likely to stay fairly steady. That said, we are trying to keep things from rising further and going back into high R values -- or in our rural area, venturing into high R values for the first time.
To compound the impression that there aren't any deaths, there is always a lag time between cases and deaths. Some of that, even with perfect reporting is built in because it takes time for people to be infected including the incubation period, fall ill, possibly wind up in the hospital, get treated, and then either recover or not make it. With further variations in when deaths are reported or recorded, there can be additional delays. There is also speculation that much of the more recent case growth is arising from Memorial Day and subsequent activities that younger people have been more likely to engage in. They are in fact less likely to have an adverse outcome, but, just as likely to pass the infection along, meaning that you also have to add one or two recurrence intervals (the time between when one person gets infected and when a person they infect starts their course) before it gets to other more vulnerable members of their household or community. With the end result that sometimes case increases are not followed by death increases for anywhere from 2 to 6 weeks. So, true, the death rate in PA has not started to rise again yet, and we want to work to keep it that way!
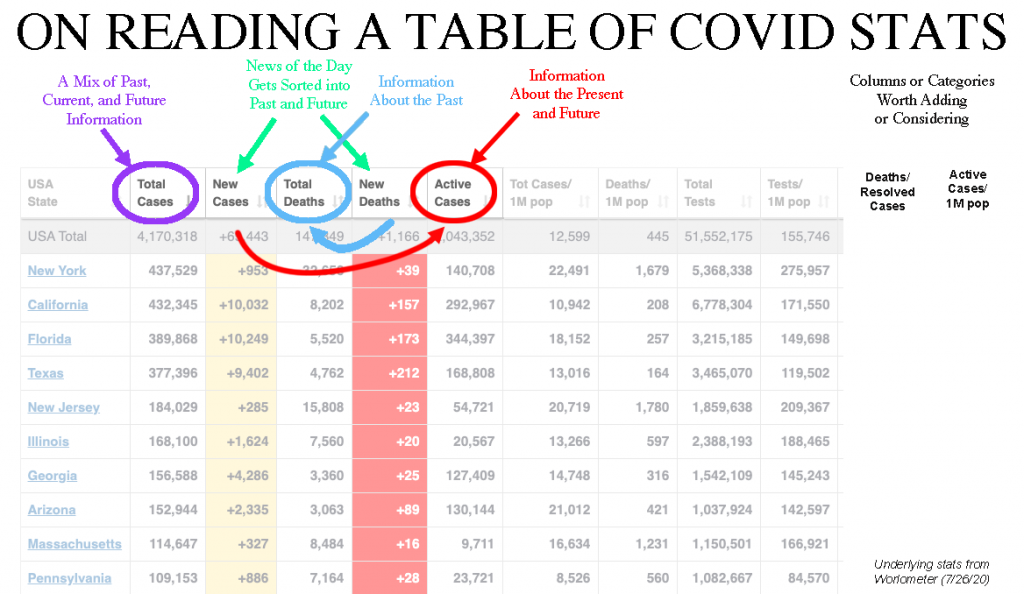
This can be seen perhaps more dramatically recently in Florida, where some public figures wondered in mid-July why the governor wasn't being congratulated on doing a better job than NY, especially in that he had a huge number of cases, but a relatively low number of deaths. That's where the words "so far" come into play. In that case it is instructive to look at how we read all the stats scrolling past us daily. Take this table (below) from Worldometer's COVID-19 reporting for the US. On any given day (in the picture the stats are from July 26), there are two highlighted columns, one of new cases and one of new deaths. These both include new information for that day, but their content doesn't really belong in the same category with each other. The new cases are about the present and the future. The newly reported deaths are about the past. You can literally imagine a person who has just been diagnosed and now looks ahead to getting through the illness versus a person whose (possibly long) course of illness has just ended for the worse. So while the total number of cases is the default sorting column for the table (at the time putting NY at the top, but now featuring CA, FL, and TX in the first three slots), it is not the most illuminating of stats. The huge number of cases NY has had has been largely in the past. Their active cases are now in the 70K range, whereas FL has resolved fewer than that. It may be more instructive to look at the deaths/resolved cases number and the active cases/1M population. It's also tempting to then extrapolate and come up with a projected number of future deaths simply based on the death rate to date in the state and the number of active cases listed. This is a very crude measure and wouldn't qualify as a model and probably it would be best to just consider these other stats as indices rather than predictions. But you can see how if you read this table as a fixed and final record of something that was already done, you might come to a different conclusion than if you read with more of a sense of the timing implicit in the numbers presented...
To further complicate things, the columns in the Worldometer table of country stats are different and in fact list Total Recovered as well as Active Cases. And number of Critical. This can make it more challenging when trying to compare from a country like Spain to a state like PA in trying to keep things apples to apples...
QUESTION 3: I have a couple questions: 1. Why are you not making any distinctions in recommendations between rural and urban areas despite the fact that even if we are legitimately seeing second wave reopening spikes, we continue to see urban areas as hotspots in terms of cases and deaths per capita compared to rural areas. Even in our own county we see anecdotally that more populated areas mask at greater frequency.
ANSWER 3: Rural areas are also vulnerable. We just have the benefit of plenty of foresight and time to take precautions, if only we would avail ourselves of it. There are plenty of examples of rural areas where disease transmission has taken off. Rural GA, OH, OR…

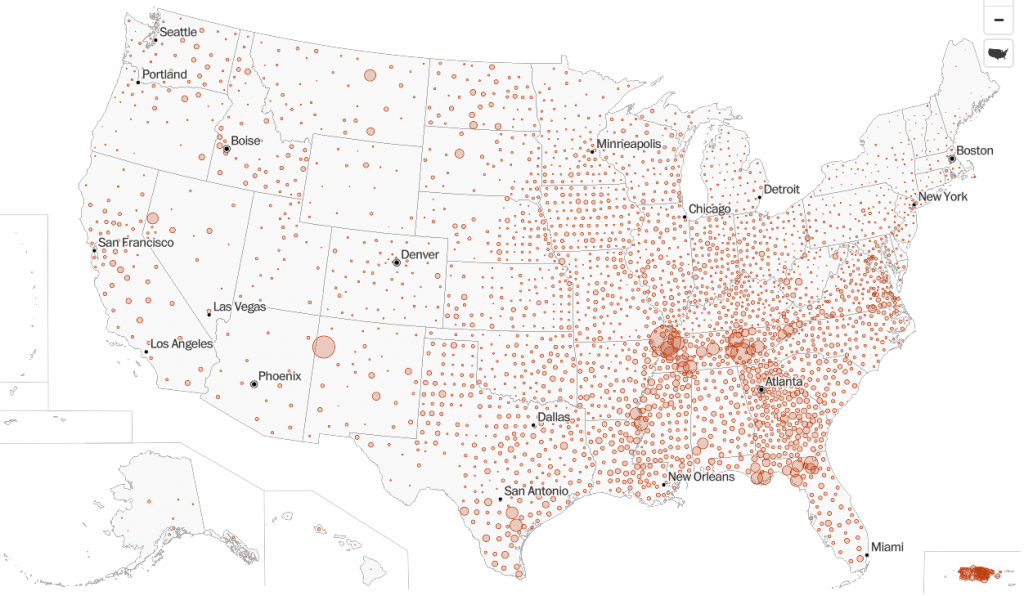
This is easier to see across the country if you review the national map of cases and death offered by the Washington Post. It allows you to toggle between totals and the per capita numbers. You can see that rural areas are also getting hit. They don't have as many numbers to add to the overall total in any given place, but plenty of rural places are being hit hard. https://www.washingtonpost.com/graphics/2020/national/coronavirus-us-cases-deaths/
For other renditions of this, check out this comparison tool looking at rural spread between March and July: https://hac.maps.arcgis.com/apps/StorytellingSwipe/index.html?appid=89420b5a3527452392b29865b006c717
Or this map from Johns Hopkins University showing confirmed cases by population:
https://coronavirus.jhu.edu/us-map
If you toggle to deaths on many of these, you may feel that in spite of the cases, they have a lower fatality rate, but remember again that deaths lag cases by a fair interval. So, as the growth in rural cases is picking up steam now and there are certainly rural counties with their share of COVID-19 deaths, many of them will play out over the next weeks and months (and longer as we continue to dicker over whether to make adjustments to slow the spread or not).
QUESTION 4: 2. In the letter to the DI, you combine masking, distancing and hygiene together as simultaneously necessary, yet in the post, Trump is lauded for recommended Masking when distancing isn’t possible? Are you saying the same thing as Trump and CDC or are you raising the bar?
ANSWER 4: To quote the president on masks plus other mitigation measures: “We’re … asking Americans to use masks, socially distance and employ vigorous hygiene - wash your hands every chance you get while sheltering high-risk populations. We are imploring young Americans to avoid packed bars and other crowded indoor gatherings. Be safe, and be smart.”
Everyone is being asked to apply these mitigation measures to the situations they are in. Many situations will call for a combination of measures. For example, the movies in the park sponsored by the Campus Theatre in Hufnagle Park on Monday nights include a combination. People are asked to wear masks to the event and to keep them on when they are moving around and getting situated and to use stepped up hygiene, including hand sanitizer made available at the event. Once they are seated, with distancing, using the spacing cue provided in the form of park picnic circles painted in the grass, they can take off their masks while they watch the movie. So they are at that point distanced, and outdoors. If they get up to move around or visit the portapotty, they should put on their mask and use extra hand sanitizer. I'm spelling this out in rather excruciating detail, but I think perhaps you get the idea.
QUESTION 5: Yikes. Does this apply to protests?
ANSWER 5: Protests do not get a pass. Protesters, like everyone else conducting their daily lives, should be wearing masks, distancing, using hygiene, considering their risk factors, and adjusting their other behaviors in light of potential exposure. If you have been in a protest or perhaps spent time on a crowded boardwalk or in business establishments at the shore, you may need to consider reducing travel and limiting contact with others for 14 days following.
The simple fact that protests are outside is the single biggest mitigation factor in their favor. But masks in those settings are also key. The question of whether people should be disallowed from being in the streets is not as clear as opponents of the protests seem to think. Cities and towns in PA or elsewhere are not shutting down as soon as there are more than 250 people on a given street. That can happen during a protest, or in cities, just during an afternoon. We aren't on lockdown right now; people have the right and the ability to be out and about. Taking the same group of people and taking their masks off, putting them close together, and indoors would be a huge risk, but unless there is substantial known community transmission, it should be feasible to be outdoors, masked, and distanced.
In fact, under the current airborne pandemic circumstances, enforcement tactics used against people who are exercising their first amendment rights demonstrating, which force them to pack together in smaller areas, force them to remove their masks, and threaten them with an even more risky ride in a police car to a station to be locked up indoors with strangers without distancing, masks, or hygiene could be seen as a further form of both physical and psychological threat/violence.
QUESTION 6: Wasn't most of China wearing mask already due to pollution before the Covid19? Kinda wonder how they worked there. SMH
ANSWER 6: In fact China, while having what once looked like a large number of cases has had, given its enormous population, fairly few on a per capita basis. It is currently ranked 27th in terms of total case numbers per country and 193rd in terms of cases per capita (58 cases/1M). They are around 160th in deaths per capita (3 deaths/1M). So, along with other things, it looks like their mitigation measures, including masking, worked fairly well. Even if China has suppressed info and has had 5 times as many cases and deaths, they are still way down the chart in terms of per capita impacts, that would put them at below 6th in total number of cases, and around 150th in terms of cases per capita, right next to New Zealand. Or maybe they are really holding back on the actual numbers on deaths; let's say they undercounted those by a factor of 10. In that case, they would still be ranked 88th in the world in deaths per capita, right next to Iceland.

