
TL;DR (too long; didn't read) Summary:
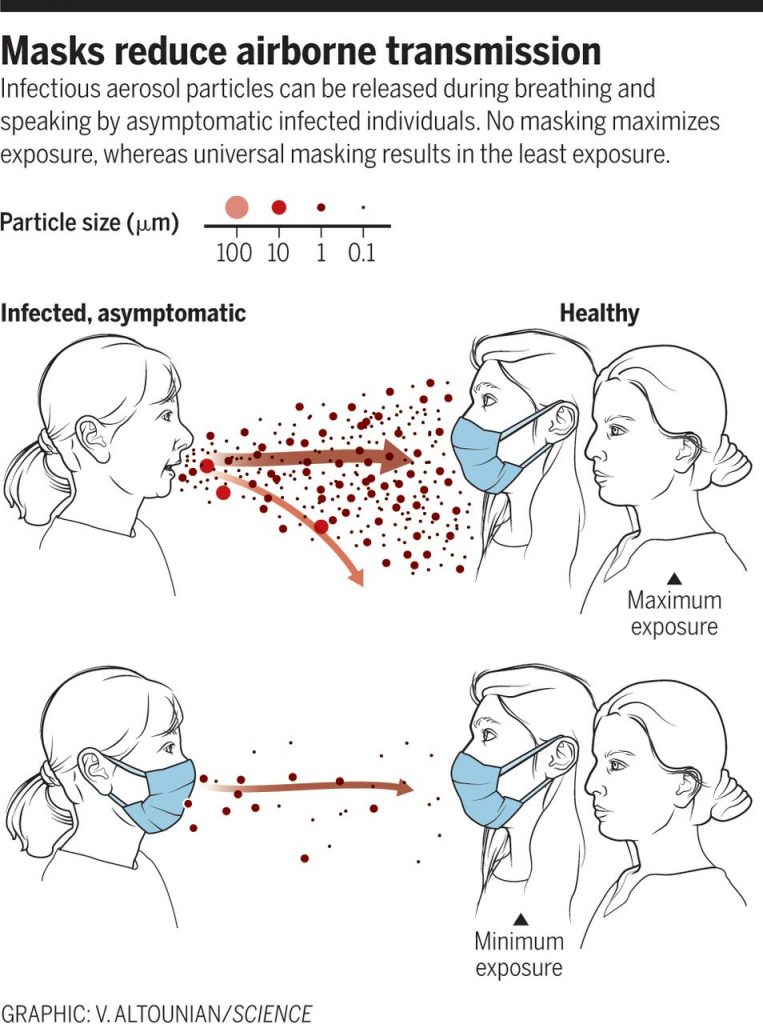
- Cloth masks are good for protecting others from the wearer; not as good at protecting the wearer from others
- "My mask protects you; your mask protects me" does not work if too few people are willing to wear masks
- We need 80% mask wearing and are nationally under 50%, with lots of transmission
- Since so many people are not wearing masks when they need to, those who are wearing masks need better protection for themselves -- look for multiple layers, high filtration, and tight fit (double masking can help with all of those)
- The new variants are more contagious and make this even more urgent during the next few months as we work through the long process to get enough people vaccinated to achieve herd immunity
- Look for KN95, KF94, FFP2, or medical/surgical masks -- check to make sure they meet the protection standards on the FDA Emergency Use Authorization website
- If you work in a high-exposure occupation (like those listed in the Phase 1B Vaccination category) and live in Snyder, Union, or Northumberland Counties, you can get some KN95 masks from the Greater Susquehanna Valley United Way
Long Version (lots more on all of the above):
We have continued to flog mask wearing for most of the past year pretty continuously (our first mask post was almost nine months ago to the day), but we have not revisited the subject in detail in a while. While much of the early information holds up, there are some new things to consider, principal among them, the need for better masks. (Essays from Zeynep Tufekci provide perfect bookends for this discussion in fact, first laying out the case for universal masking to protect others and now insisting on the move to more serious personal protection.) In theory the homemade masks were a last resort, a stopgap to be put in place to buy us all some time to get more effective protection in place. As we've been hearing all along, cloth masks are good enough to help us flatten the curve. What they would be good enough at would be protecting others from the wearer. Remember "your mask protects me; my mask protects you"? They were good at protecting other people from the wearer (outward protection), but not particularly good at protecting the wearer from others (inward protection). And studies had shown that we needed approximately 80% compliance for the protection to work -- we have fallen short!
So in the absence of the universal part of universal masking, those of us waiting for the more engineered, inward protecting options to come on line have had a long and lonely vigil. It does look like there is movement on that front, but it's coming about six months late, twelve if you consider the fast action on this topic on the part of Asian countries like South Korea. The identification of multiple genetic variants of COVID-19 that appear to cause similar levels of acute disease but are more easily transmittable has also brought this issue into stark focus once again.
We finally have vaccines, but it takes time to get them into people's arms and then allow them to work their scientific "magic" of priming the immune system to effectively squelch the severity of the target virus. The new more infectious variants are upping the virus' game and spreading infection faster, both getting more people sick AND increasing the chances of further mutations that could work to the virus' benefit and our detriment. (Viruses are always mutating, but many of those mutations either don't matter or actually hurt the virus. The trick is every replication is a lottery ticket and allowing the disease to spread so widely is like buying the virus a massive bounty of lottery tickets. Give them enough random chances and eventually they are going to come across a winning ticket.)
So now it's a race. We humans need to hold off on getting sick just long enough to get to herd immunity through vaccinating roughly 80% of the population in any given community. Even working at breakneck speed and with laser-focused efficiency and superlative reach, it's going to take months to get that many of us vaccinated. The previous White House's Coronavirus Task Force has been reporting since early December that we will need to get at least 100M of the most vulnerable in the US inoculated before we can substantially start to reduce the spread and slow down the deaths over the long term.
Meanwhile the virus is honing its tools and starting to plow through populations ever faster. We've long known that only a fraction of those infected have been responsible for most of the spread. It could be that the genetic changes cropping up now make those same people more infectious or they might make more of the people infected more likely to spread it. Variants along these lines have been identified in the UK, Brazil, South Africa, and California so far; those are just the ones we've been testing for enough to find... People infected with them may be producing more viral particles or the virus may be better at getting embedded when it encounters a new body to infect. Whatever the mechanism, the timeline is inexorable and in the months it will take us to vaccinate large numbers the disease will be marching along, infecting people, incubating in them, and getting shared with others even as the previous round of hosts are still just starting their course of symptoms. It seems to take around 5 to 7 days from the time of exposure to the peak of infectiousness and the start of symptoms. There's time for a lot of generations of disease while we're racing to vaccinate.
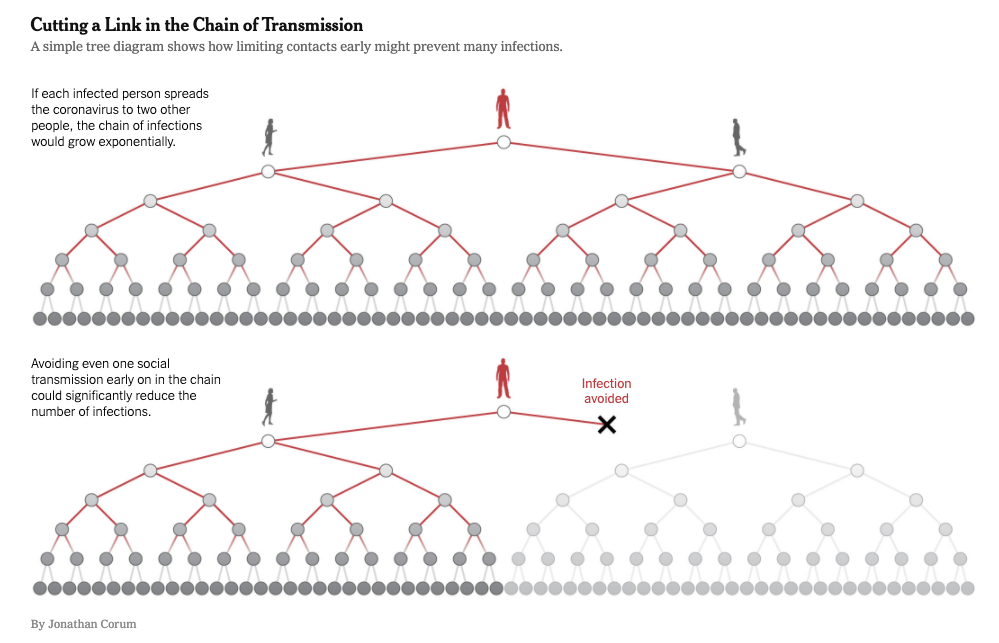
We need to cast our minds back to some of the very early graphics showing us the importance of interrupting transmission chains and how refusing to become a vector can potentially protect huge numbers of people "downstream" from us.
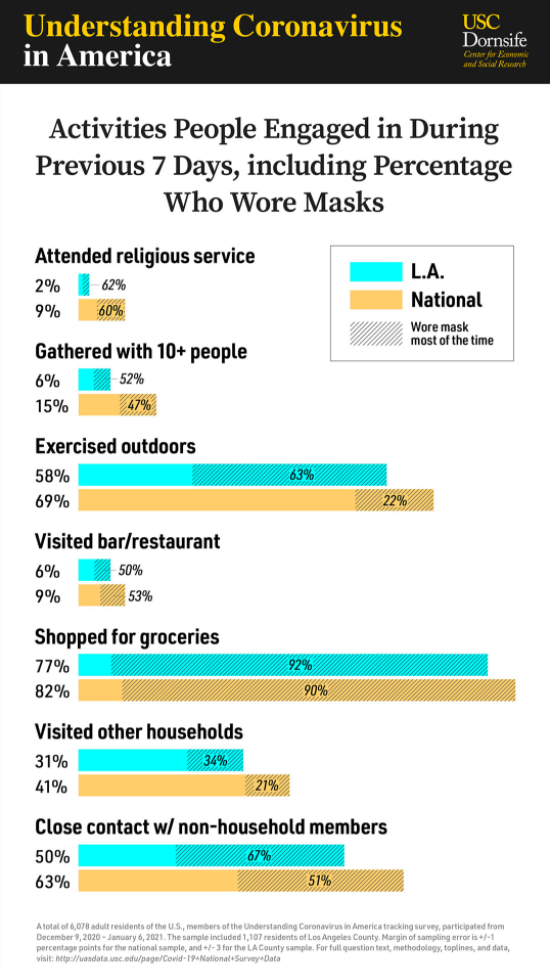
So, other than vaccines, how do we interrupt that transmission right now? Masks, distancing, hygiene, avoiding indoor gatherings, and isolating if positive, exposed, or symptomatic. Sounds familiar, right? If we've known this all along, how can this be the solution? Because we aren't necessarily paying attention to it. A new study came out just this week looking at mask use in a variety of situations around the country and concluding that about 50% of adults are not wearing masks when they should be. Locally, one can confirm this using the "any fool can see" research method...
So a lot of us have been following the guidelines, but maybe not all the time, and some of us haven't been doing any of them at all. It's time to do better.
What are we to do about those who have for a variety of reasons dug in their heels and refuse to do what's necessary? Well, since we are having so much trouble with source control (universal masking to keep asymptomatic and presymptomatic carriers from sharing their germs), it's time to give personal protection another look.
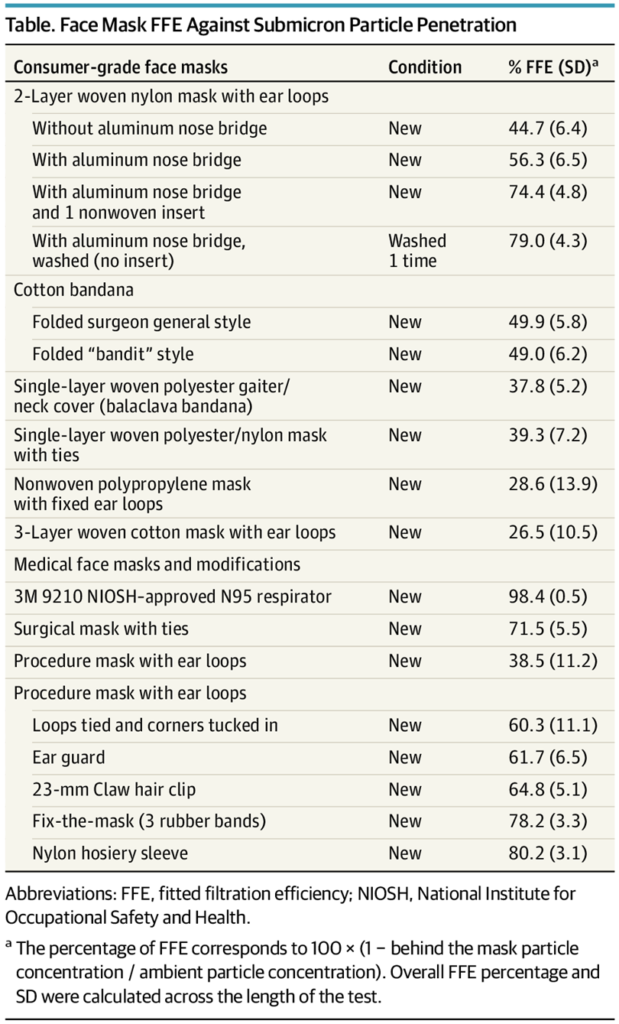
There are new studies out about how well different types of masks work as PPE, i.e. for protecting the wearer as well as those around them. In those studies cloth masks and bandanas do not rate particularly well. (Though adding filtration, as was suggested early on, and ensuring a tight fit, could do a lot.) The cloth masks can also still be useful as a protective and supportive layer for other more effective filters. In other words, double masking is a thing. And it may help your KN95 or KF94 mask last longer.
This is the way we move forward and stop having existential crises about situations where we must be around others who refuse to do their part, whether at work, or school, or the post office. We need to protect ourselves if people are not willing to protect the community they are in. This still begs the question of all the people who have no choice about who they must interact with: grocery store workers, teachers, hairdressers... Hopefully people who are acknowledged as being at greater risk by still being somewhere in the Phase 1 tier of PA's vaccination plan will soon get access to real PPE, because that timeline is stretching out ever longer, especially as more and more people get frontloaded into the 1A category.
None of this is an indictment of cloth masks or those who made them so diligently or those who continue to use them. Nor is it meant to accuse those deciding on the order of vaccine eligibility of anything nefarious. It is simply a recognition that COVID-19 is upping its game as we move into crunchtime and we need to do so as well.
As things stand, there are KN95, KF94, FFP2, and surgical masks available on the market currently. It is possible there will be an effort to distribute these more effective masks more broadly and to increase production to make that possible. It is still not clear that even healthcare workers have enough PPE at their disposal from day to day, so we should continue to reserve N95s for medical use, but the others are at least on the shelves and in stock. (KN95 is the Chinese version of N95, which seems to be somewhat less durable and sealing, but still a big step up from handkerchiefs. Beware of counterfeits though; look for ones certified by the FDA with an Emergency Use Authorization. KF94 is the South Korean version. It is referenced by reputable sources like Dr. Ashish Jha, but does not appear in the PDA EUA lists. We will update if we get more information about their certification. FFP2 is a European certification.)
So let's get serious and start using all the tools at our disposal for ending the pandemic. Some interventions will be pharmaceutical, like the vaccines. Some continue to be individual, like homemade masks and personal behavior change to practice distancing, avoid indoor gatherings, and isolate if positive, exposed, or symptomatic. And some could be medical-grade physical interventions that the powers that be need to ensure production of, make sure we can obtain, and encourage us all to put to use -- like high filtration masks. But the first step is understanding that they are needed!
VACCINE/MASK CODA
Maybe you're in the ever-growing Phase 1A vaccination group here in PA and you figure you're not that far out from full coverage (roughly two weeks after your final injection) and are looking foward to busting out. Not so fast! You are still going to need to mitigate. Whaaaa? It goes back to that little thing we've been worrying about for so long, asymptomatic spread. The vaccines do a very good job of protecting the vaccinated against developing severe COVID-19. It is not however clear that those same people can't still be carriers of the disease and infect others, even as they are protected. In light of that, until we actually get a large percentage of the community vaccinated, those lucky enough to already have their shots will need to continue wearing masks, distancing, and avoiding indoor gathering...
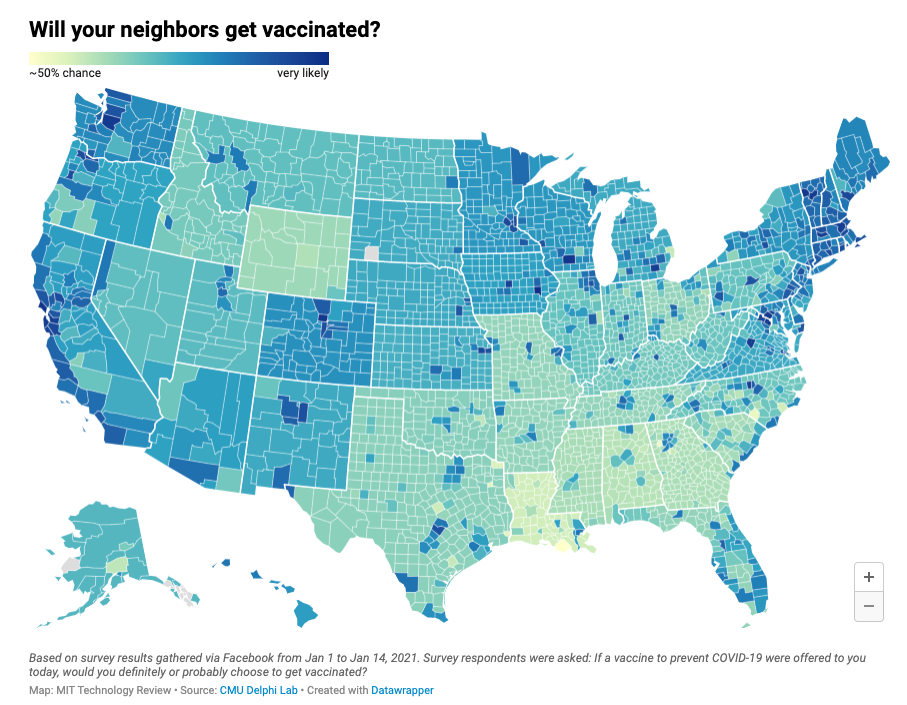
Observant readers will note that the estimated level of vaccination needed in a community to eliminate the risk of COVID-19 is around 70 to 85%. Feel free to compare that to the numbers of people currently expressing interest in getting the shots in the map above. Time to get to work on another round of public health messaging. Please talk to your friends (and enemies) and pastors and associates and your distant relatives and your kids' friends' parents and...
In effect, the vaccines are going to create an even larger percentage of asymptomatic cases than we are currently facing! And a new bifurcation of experience. We have long had people ignoring public health recommendations and those following them. That will intensify with the willful ignorers joined by less conscientious already vaccinated folks. Don't be in the latter category. Love thy neighbor please!
PS Don't even talk to me about face shields. Yes, it's good to cover your eyes. No, they don't do much of anything in terms of protecting either you or those you interact with from anything but the most substantial of droplets. They are aerosol free-for-alls. If you have to be indoors around someone who insists on only wearing a face shield, get yourself a decent KN95 mask and try to spend as little time in their presence or in rooms they frequent. In case they're interested (hahahaha!), you could let them know that face shields are recommended for use in combination with masks.
