
Where do we stand right now? Places that have been tracking the numbers over the past year plus have been revamping their data pages recently. It's time to integrate infection and vaccination data, rather than looking at those things in isolation. So, looking at all the number tracking, what is really going on in Union County at this point?
As of May 6, we see that we have had approximately 6000 confirmed or probable cases in the county. We also see that we have about 12000 people fully vaccinated and another 4700 partially vaccinated (though that could mean first shot given two days ago). Allowing for the fact that a fair number of the people vaccinated were also among the number of reported cases, we could say that we are likely at a minimum of 33% with some degree of immunity.
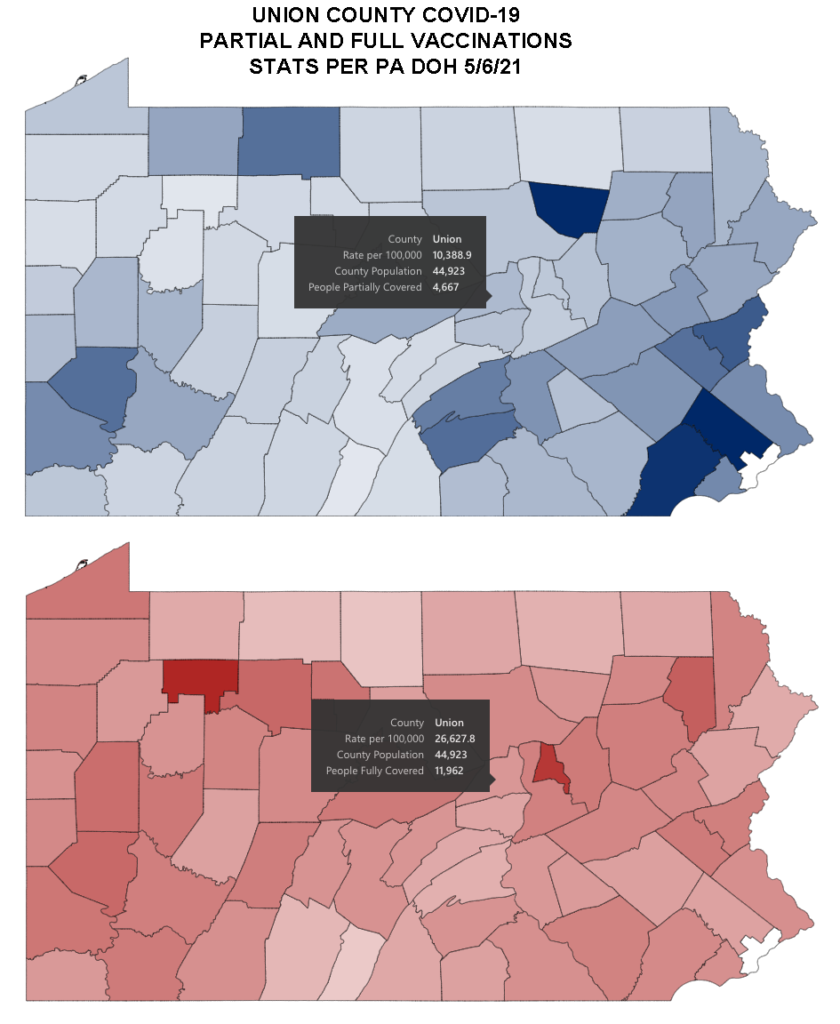
We can also allow that because of a variety of factors whether lack of access to testing or asymptomatic cases or resistance to disclosure, there were many additional cases that went "under the radar." Over the course of the entire year, those are unlikely to have been greater than twice the number of reported cases in our area, but even if they were at that high mark, that would mean we could estimate something like 18000 total having been infected (as opposed to the 6000 known to have been). And being optimistic both about the number of people partially vaccinated who will finish their course of shots and the promptness of that process, we could add in the 4700 to our current number of vaccinated. And we could further pad things by assuming no overlap between those infected and those immunized, giving us a total of 34700 with some kind of immunity. That could get us to 77%.
But that's only with some very generous assumptions. We are likely somewhere in between 33% and 77% with some measure of immunity. Splitting the difference puts us around 55%.
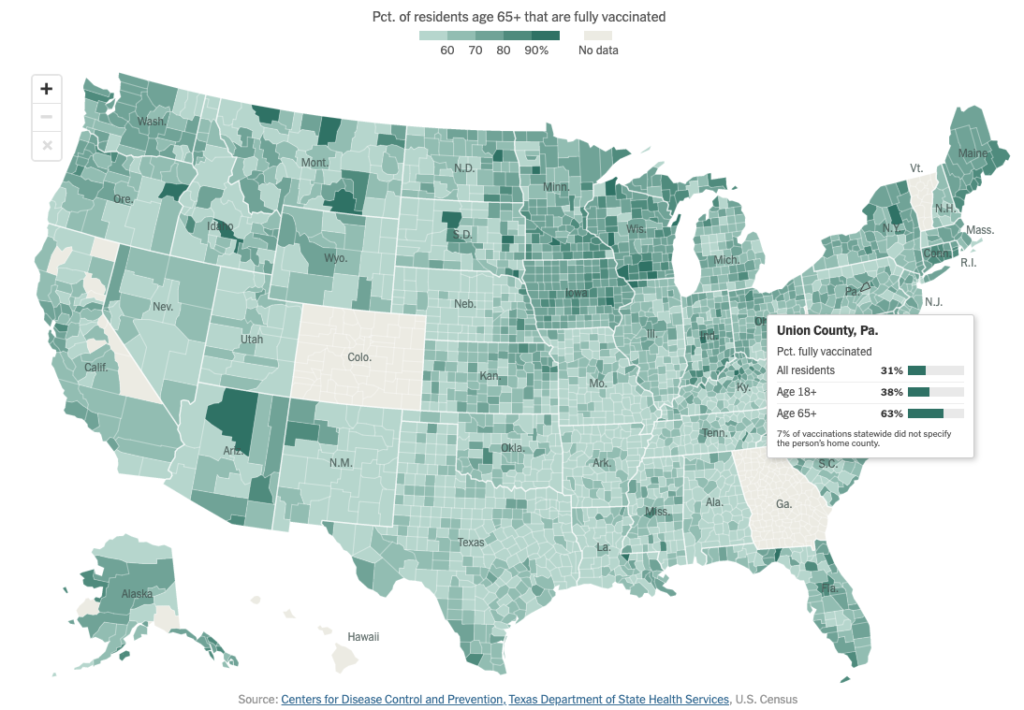
Yes, there's a good deal of guesswork involved. But the point of the exercise is to illustrate that having whatever the number is for the county -- 31% of all residents, 38% of those 18 and over, and 63% of those 65 and up (according to NYT reporting for 5/6) -- vaccinated thus far does not mean we are done yet. Not to mention that this is a global epidemic and we are still subject to the vagaries and vicissitudes of viral transmission continuing in some places almost unchecked right now. And the immunity afforded by getting infected directly has been seen to be less dependable than getting vaccinated.
We should acknowledge that the curves we are looking at this spring even if they look similar to curves from other times in the last year mean something different. Last fall, we had to point out how the drastic changes in the availability of testing meant that it was not possible to read directly across on the graphs and compare confirmed case counts from Spring 2020 to those in Summer or Fall of that year. Now, we need to look at those same cumulative case count graphs and factor in the reality of increasing immunization. Even as cases go up on similar trajectories to those in the fall, and hospitalizations rise, we expect the final tally of deaths to be far less brutal for similar numbers of reported cases now. To that, we should point out that variants are working to make all the prior conferred immunity moot -- the more cases, the more opportunities for opportune mutations. And there is no guarantee that the risk profile for variants will be the same (recall that the 1918 Influenza had the greatest impact on the 20-39 age group, as opposed to the very old or the very young).
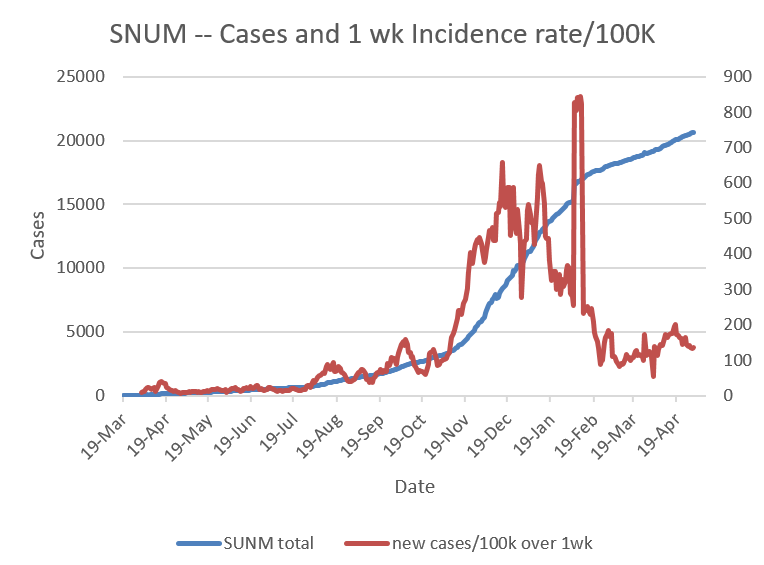
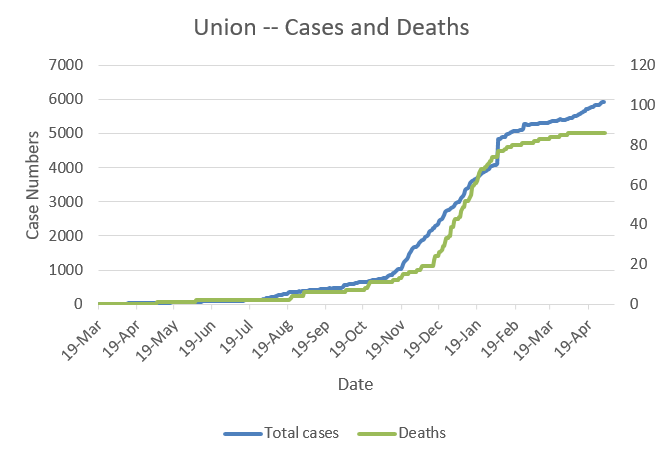
New case rates dropped slowly from the beginning of the year to the middle of March and then rose slowly to the latter half of April. They are a bit lower again, but still above the maintenance levels from 2020. Hospitalizations also rose and deaths continue to bump along at a low level, but higher than we saw during most of 2020 until the November/December spike. In addition, the test positivity rate has been fairly high since mid-April which seems to indicate that there are even more cases not being captured.
What this means is that more people locally are carrying and circulating the disease than were up until November 2020, but that many of the people most threatened by this have some measure of protection. It also means that we are continuing to conduct an experiment with slightly less dire consequences, but that we once again don’t have a great window into what said consequences will eventually prove to be. It looks like the case and death graphs may be diverging finally. Based on real-world data from Israel which launched a very aggressive vaccination program starting in early December 2020, once we get to 40% vaccinated, a significant divergence in deaths with respect to cases is noticed and cases themselves drop off at 70% vaccinated. (Vaccinated, not vaccinated or infected; there is too much variation and lack of data to assess that from country to country.)
Are we in fact now starting to bring this infection more into the realm of being like the flu as so many have insisted (in the face of evidence to the contrary) over the past year? Some remain fixated on the vaccination levels for those "most at risk," i.e. 65+ years old, and maintain that once they are vaccinated, it's over. But let's remember that that really means "most at risk of dying" and that there are plenty of ongoing impacts from COVID-19 already starting to come to light that those who do a better job of surviving are still suffering from. A recent study from the Lancet notes that up to 75% of those diagnosed (not just those hospitalized or otherwise seen to have severe cases) are having neurological impacts 6 months later. This study covered over 200k people diagnosed with COVID-19, not a small sample. Even if the diagnoses lagged by half, that's still more than a third of people infected and surviving having longterm side effects affecting their mental function. And that just looked at neurological function. Other studies have examined long term impacts on the heart, the lungs, and the circulatory system. All in all, not exactly something we need to be signing up for. And also not at all like the flu.
We also know that neither "natural" immunity or induced immunity from the vaccine is airtight, though the vaccine does appear to provide better coverage. There are reported cases of reinfection and breakthrough infections, so what we would really like to see is the amount of virus circulating in the community brought further down.
As predicted, there are now lots of opportunities to get immunized. It is free, easy, and there are agencies working to overcome any barriers people may have, whether they need help booking an appointment or assistance with transportation. Also as predicted, there is substantial reluctance or hesitancy to getting vaccinated. What we need to remember is that vaccination offers protection at the level of the population. An individual vaccine is a step along the road to herd immunity but does not in itself get us there. The new proposal on the part of the governor indicating that once we get to 70% vaccinated, we can remove the mask mandate is making a stir (as is the less talked about possibility that between those not eligible to be vaccinated, like children and people with immune deficiencies, and those refusing, the hopes of getting to 70% are diminishing, especially on a local level).
We may soon be really delving into the numbers and working to tease out the differences between the state Department of Health reporting versus CDC numbers (which seem to involve including or not including Philadelphia which has its own vaccination distribution and tracking regime and may also reflect different total population assumptions now that updated census numbers are coming in) as we try to eke out achieving 70%. The Daily Item's math seems to put it within reach, noting that while only about 27% are fully vaccinated in the county so far, the state is closer to 42% (though as mentioned this figure is at odds with the 34% shown elsewhere). And those who are partially vaccinated will, once (if) they finish their course, bring the state up to 63%. In that case, maybe our local/rural posting of poor numbers will slip by?
The people who are most reluctant to get vaccinated comprise a significant portion of the population in this region. They reportedly do not want to hear about needing to get vaccinated. They don't want to hear about it from politicians of any stripe. They say they just want the facts, though they haven't seemed particularly interested in those either. In theory, their family physicians may have the best chance of communicating with them about it (though in this region, they may be getting support in their skepticism from some of those very doctors -- not the vast majority... but some). It might be good to recall here that pressure campaigns by close family members actually can tip the balance. Partners, children, and other relatives both normalizing getting the vaccine and insisting their fathers, uncles, sons, nephews, and cousins get it or at least talk to their doctor about it, too, can make a difference.
In the end, terminology is not immutable. Hesitancy is just that, a delay, perhaps soon to be overcome, maybe through enticements like the $100 savings bonds West Virginia is offering to young people who get the shot or cold hard cash being offered by some employers as inducement. It doesn't have to be a permanent, hardened refusal.

In about six weeks we will likely be in a different place -- one that a lot of us have been trying to get to for a long time. By then people who want to support the public good of striving safely for herd immunity will have largely been vaccinated. Same for those who want the personal measure of protection afforded by the vaccine; they will have had the opportunity to get it. At a certain level at that point, those who refuse will have made their own decision and will take their chances. Unfortunately, there are consequences for many people other than those self-styled rugged individuals. There are people who are unable to get the vaccine either because they are not yet approved for their use (children) or because they have other contra-indicators (severe allergies or other immunocompromised conditions). So while the world has long been fraught and full of potential threats for people in those categories, others choosing not to get immunized against this particular disease will leave them in ongoing isolation.
It also means the disease is likely on its way to becoming endemic, rather than eradicated. It will continue to circulate, and we will continue to have to make provisions to fight it off, as we do with the flu. There may be boosters at some interval, every year? 2 years? 3? We don't know yet. Plus as mentioned increased hazard for the more vulnerable... And that extra danger once again in turn can impact all of us. Not only does the virus get lots of chances to replicate and mutate with each new person it infects, it also gets to have a field day once it manages to lodge itself in the system of someone whose immune system really can't fight it off. The B.1.1.7 variant, for example, seems to trace back to a lingering months-long infection in one man in northern England with a compromised immune system. Too bad the rest of us didn't do a better job of keeping him -- and ourselves -- safe!
All this is to say that it seems like we can acknowledge some misgivings but also weigh not just our own chances but the impact on our family, friends, and community and come to the conclusion that it's time to get vaccinated -- for their sakes. It wouldn't make you any less hearty or feel any less invincible (possibly more even!) but it would mean you were more caring and protective of others. The best advice we can probably give is that if you have questions, go ahead and ask them, not of a search engine but to your family doctor!
"Ask your doctor if the COVID-19 vaccine is right for you!"
Vaccination is the safest route to herd immunity. Our community can get past the frustrations of the past year with something now readily available to us. We would all probably prefer a magic wand, but perhaps we can squint and reimagine the syringe as the magician's implement. Let's do this!

