It's late January 2021. You may be asking yourself what is going on.
Well, things are pretty intense right now. Tensions are running high. As is confusion.
Lemme ‘splain.
The vaccine rollout landscape shifted on January 19 when the previous administration recommended states add everyone over 65, plus younger people with significant COVID risk, to their priority vaccination tiers. In PA, that meant expanding Phase 1A beyond healthcare workers and nursing home residents and employees (not all of whom had or have yet been vaccinated) to include an additional 3.5M people. 1A had been a little under 1M to start with. (Observant readers may note that that brings the total in the first priority tier to a third of the population of the Commonwealth -- and an even greater proportion of the vaccinate-able, since those under 16 are not anywhere in the queue yet.)
There was no increase in the supply of vaccine provided to match the expanded demand.
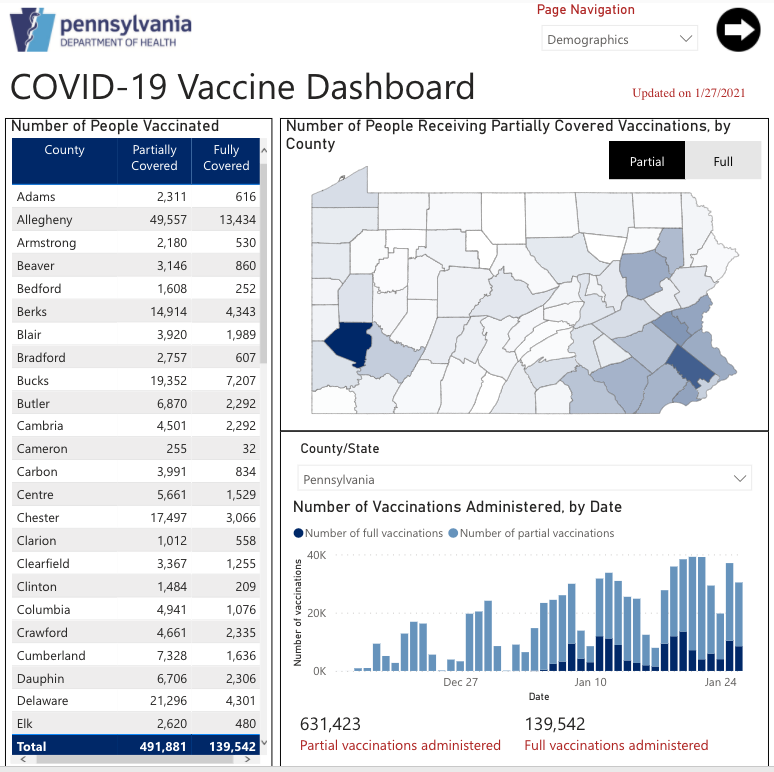
As of January 26, the Commonwealth had partially vaccinated over 600k people and fully vaccinated almost 150k. That’s basically twice as many as had been vaccinated as of January 19 over the previous month of vaccinations. So, allowing for those that have demurred in the initial 1A group, they are getting pretty close to having administered the total number to be expected in that group. However, because of the expansion, there are many people now starting to be vaccinated who are in the newly eligible categories. This means, as of now, not everyone in the initial 1A group who wants to be vaccinated has been, particularly nursing home residents. They really should continue to be a high(er) priority – call the newly eligible Phase 1A’ if you have to.
As mentioned above, while the previous administration pushed states to expand eligibility, they did not ensure vaccine supply to match. So the current traffic jam of people trying to figure out how and where to get signed up for vaccination was pretty inevitable. Put it this way: 3.5 million Pennsylvania residents were added to phase 1A, but the state has only been receiving about 140k doses per week. We do expect the number of doses available will rise significantly in coming weeks AND that vaccine providers will get clear indications of how much they will be receiving 30, 60, and 90 days out. Both of those are explicit goals of the new federal COVID-19 Team. Once we get there, getting people signed up for appointments (and getting duplicate appointments cancelled!) and moving people through the pipeline should work much better.
There is a lot of angst and frustration right now being directed at anyone and everyone involved but ironically the current mess was primarily created by people who are no longer involved at all. For perspective, at the rate of delivery indicated above, it would take 12 weeks for the redefined Phase 1A to receive all their shots. Clearly, supply needs to ramp up!
People have noted that there are some people in Phase 1B who have already received their shots in various parts of the state. 1) Some people in Phase 1B are also in the expanded 1A because of either age or health history. 2) There has been some pilot 1B administration and that hasn’t been consistent. 1B includes people in jobs that require significant exposure over which the workers have little control, including teachers, grocery store workers, postal workers, factory workers, etc.
Remember earlier discussions of personal COVID risk factors when we talked about how a large segment of the population falls into those categories? That’s what is playing out right now.
There are lots and lots of people who really do need to get vaccinated and only so much vaccine available in any given day, but it's still good news that people are so ready to be vaccinated. Lots of people want to avoid getting COVID-19, but we can't all get vaccinated simultaneously, so we have to take turns getting our shots and in the meantime continue with the NPIs (non-pharmaceutical interventions), like masks, distancing, and hygiene only more so.
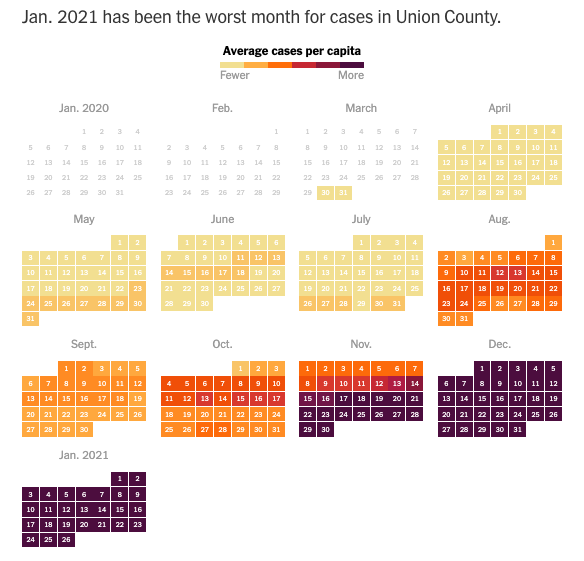
The bad news is…. More contagious virus variants are starting to crop up. While there was a dip in new cases after the holidays, possibly a function of people staying to themselves during the break, deaths continue to rise (lagging), and the dip is merely bringing us back down to a new, too-high-case-count normal, well above what has been defined as “substantial spread.”
Studies are indicating that the COVID fatigue everyone has a general sense of really is taking a toll on people’s carefulness even with the most basic of mitigation measures like masks. In fact a recently released national assessment conducted by the University of Southern California indicates that fewer than 50% of adults in the US are wearing masks in situations where they should be, even though 83% acknowledge that doing so is important. Want worse news? Mask wearing is even less likely among white people and those in rural areas even though all evidence indicates it is just as needed in those categories.
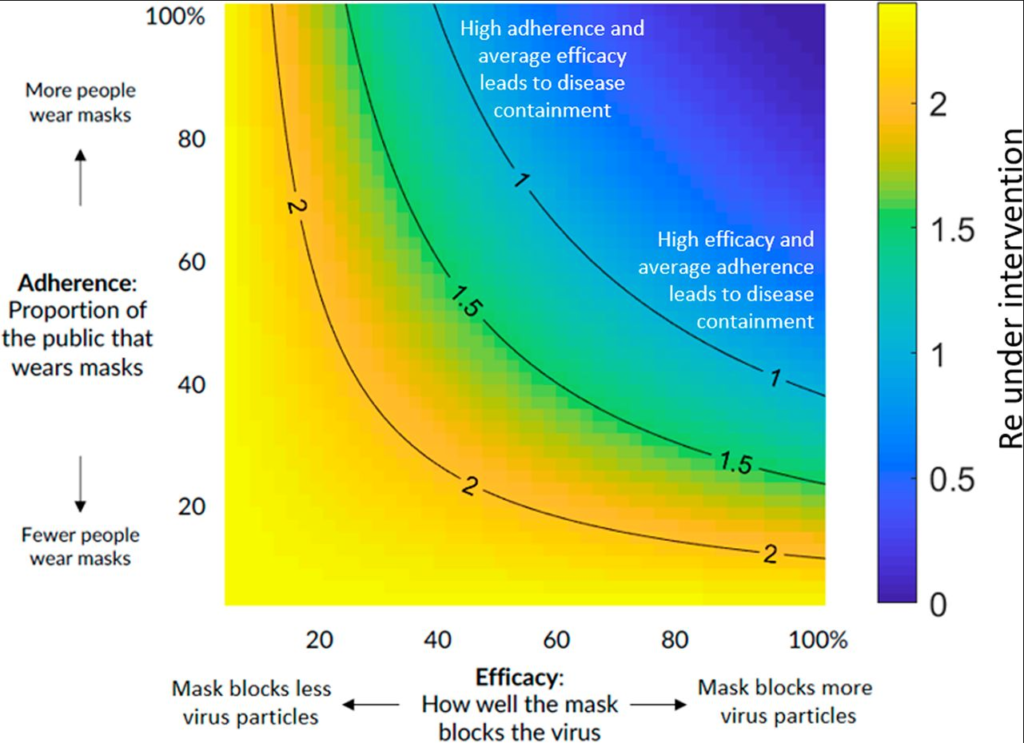
We’ve long heard that the way cloth masks are supposed to work (as source control) means “your mask protects me; my mask protects you.” So what should we do if the people we’re around are not willing to wear masks to protect others? Well, simply put, it’s time to get a better mask. The typical cloth masks many people have been wearing would do the job if ~80% of people were wearing them consistently. We are all painfully aware of how many people either refuse them entirely or wear them in completely useless fashion, whether hanging off an ear, under their chin, or with their nose sticking out.
What is a community-minded person to do? It’s time for people to recommit to their mitigation efforts in order to protect against the more virulent variant and allow vaccination to expand. Masks that protect the wearer are part of that. We should continue to reserve N95 masks for healthcare workers, but there are somewhat less durable high filtration KN95, KF94, and filter inserts that the rest of us have recourse to now. To assist the community in this and recognizing that not everyone has the resources to purchase such supplies, the Greater Susquehanna Valley United Way has procured a supply of KN95 masks that will be made available to people in Phase 1B categories to assist them in holding out as healthy until their turn comes in the vaccination queue.
We all need to double down (how many times have we doubled down? we're now doubling to the fifth...) on these risk reduction measures. They will look familiar, but updated:
- Wear masks (high filtration, well-fitted ones, worn properly! Double masking is a thing…)
- Keep distance
- Increase hygiene (the variant may be more durable on surfaces!)
- Avoid indoor gathering (wear protective masks if you must be indoors with those from other households, whether for school or work; reduce duration and proximity of exposure whenever possible – and don’t take your mask off! Take anything that can be virtual online)
- Isolate if positive, exposed, or symptomatic (there should be no breaks from isolation or quarantine other than for COVID testing or medical care; get food and medicines delivered; stay inside! If you need help with this, ask: contact the Greater Susquehanna Valley United Way or the Union-Snyder Community Action Agency for assistance)
And, when your turn comes, GET THE VACCINE!
One final (unwelcome) note: those who get vaccinated earlier will still need to continue with risk reduction for the many months it will take to get the entire community protected. The vaccine will significantly reduce the chance of getting seriously ill but may not prevent people from getting infected. It is quite likely to actually increase the number of asymptomatic carriers of the virus. That means more asymptomatic people we need to keep from infecting others, especially those who have not yet been vaccinated (the many millions of us!).